Seems like a good time to give the Red Triage treatment to some of these health issues.
So here goes our first What You Need 2 Know (WUN2K?)
How Do You Say It? It is pronounced ProsTATE not prosTRATE. To be prostrate is to lay flat on the ground face first in front of someone either because you are being arrested or really, really into religion. ProsTATE is a greek word meaning protector or guardian. Which allows for this fun sentence: "The prostate, prostrated himself before his King."
Why Do We Need It? The prostate is a gland that produces a liquid that protects the sperm from the acidic environment of the vagina.
This -- and the fact that prostate exams are conducted with a doctor's finger in the rectum -- make it hard to talk about the prostate at dinner parties.
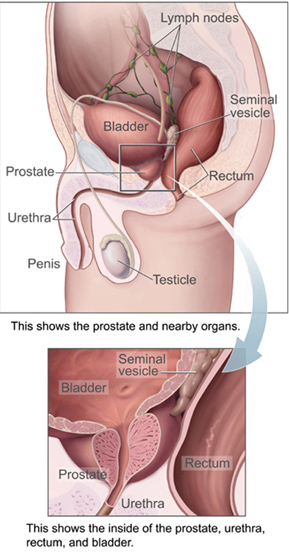
Why It Causes Problems: This is a gland that wraps around the urethra just below the bladder. So if it swells up for any reason, it makes urinating difficult. It's not really in the penis, but messing around with it through surgery can affect a man's ability to have sex and urinate. These are two things men really like to do.
Can We Live Without It? Sure, it is one of the glands a guy could get along without. It would be harder to make babies, but not have sex. The problem comes in getting rid of it. It is located in a spot where a lot of the blood vessels and nerves running to the penis are also located. As noted above, collateral damage is possible and can lead to problems having sex and urinating.
What is Prostate Cancer? Think of cancer as runaway evolution starting with one cell that has an error in its programming. It reproduces like crazy and makes more bad copies. These cells can sometimes spread to distant parts of the body. Different cells make different kinds of cancer and those cancers cause different kinds of problems and symptoms. They act differently. Some causes big problems, pain and death. Some cause minimal problems and there are probably cancerous growths that are never discovered and are handled by our bodies defenses.
Nowhere is this more evident than in prostate cancer. There are different types - a slow growing kind and more aggressive, fast growing kinds. It has been said that most of us men - if we live long enough -- will probably die WITH prostate cancer, but not FROM prostate cancer. That's because the slow growing kind of prostate cancer is much more common. This kind does not spread to other parts of the body or mutate like the more aggressive types.
Lies, Damn Lies and Statistics:
Prostate cancer is the most common cancer in men.
It is the second leading cause of cancer death for men in the United States.
An estimate 238,590 men will be diagnosed this year.
Approximately 29,720 will die from it.
Survival rates are good with 98 percent surviving 10 years after diagnosis and 93 percent surviving 15 years after diagnosis. However, while death from prostate cancer is declining among all men, it is still twice as high for black men than white men. (source, American Cancer Society via Cancer.net ) Black men have a high incidence of prostate cancer and tend to get the more aggressive form.

So, if the PSA level is high, it may indicate that a man has an aggressive prostate cancer that has yet to become symptomatic.
Or it might not.
Here's what the American Society of Clinical Oncology has to say:
In some situations, PSA testing finds aggressive prostate cancers early and save lives. However, it is not easy for a doctor to predict which tumors will grow and spread quickly and which ones will grow slowly. In some situations, men who have a prostate cancer that will never cause them harm may be discovered, and this discovery means these men will undergo additional testing and treatments that turn out to be unnecessary. These tests and treatments put a man at risk for infection, impotence, incontinence, and rarely, death. Each man’s risk of prostate cancer and acceptance of potential side effects is different.So if you are over 50, you should talk with your doctor about whether PSA testing is appropriate and if the test comes back positive, what the plan will be. New guidelines allow doctors to take a "watch and wait" approach, rather than initiate invasive testing. (For more on this, see earlier post on Medical Testing.)
How Do I Not Get This:
Don't get old (80 percent of all prostate cancer is diagnosed after age 65) and eat a low fat diet with lots of fruits and veggies. Will that prevent prostate cancer? We don't know but it can't hurt and some research seems to point in that direction.
Don't go crazy with supplements like Selenium and Vitamin E. The SELECT study looked into these and found that they not only did not prevent prostate cancer, but may have caused more harm than good.
This seems to be a type of cancer that doesn't rely on genetic inheritance, although if you have close family members (son, brother, father) that were diagnosed at a young age, your chances are higher of developing the disease.
The Jury's Still Out: One area of research is a link between vasectomies and prostate cancer. One study in 1983 showed an increased risk, however subsequent review has shown that the link between the two is very small and the increase in risk if they are linked, is also very small. Size does matter. Get the vasectomy.

![By Penarc (my own picture) [CC-BY-SA-3.0 (http://creativecommons.org/licenses/by-sa/3.0)], via Wikimedia Commons](http://upload.wikimedia.org/wikipedia/commons/b/b5/Glucose-meter_17_12_2010_012.jpg "This can save a life (photo by Penarc)")

